This week’s Sacramento News and Review featured a story by Seth Sandronsky which outlined the plight of former Sacramento resident David Bell, who worked for a Davis biotech firm, AgraQuest.
According to the the News and Review article:
“Five months later, he came down with severe flu symptoms. His face and teeth grew numb. Breathing became difficult and he developed severe headaches. His nose bled and his sputum turned bloody.
Ten years, four sinus surgeries and numerous medical treatments later, Bell remains incapacitated by the illness, which he and his mother, Sandi Trend, of Citrus Heights, claim was caused by bacteria and fungi he was exposed to at AgraQuest.”
The Vanguard has been investigating this story for the last several months and is very concerned about the possibility that some of the microbes and bacteria that were used in this lab could have escaped into the Davis environment and exposed Davis residents to potentially lethal infections. One of the problems that David Bell faced was a broken Worker’s Compensation system. The main focus of the News and Review Article was the plight of David Bell and the problems in the Worker’s comp system.
Our concern however is also with the residents who live and work near 1105 Kennedy Place, in Davis, the original location of Agraquest. It is located near two school sites and surrounded by residential neighborhoods.
At this point in time, we would like a regulatory agency to explore the area around the lab and determine whether there are possible pathogens that would represent a health risk. One of the challenges we face however is uncertainty as to who holds regulatory authority over this issue. Efforts at this time are underway to determine who holds regulatory authority and how the possibility of a health threat can be investigated.
WHAT THE LAB CONTAINED AND THE OFFICIAL RESPONSE OF CAL-OSHA
According to the News and Review:
“AgraQuest was founded in 1995 by Pam Marrone, a respected entomologist who had specialized in agriculture and insects at biotech giant Monsanto. Bell was a semester away from earning a bachelor’s degree in biology from Sacramento State when he started at the company in 1998. According to the transcript from his first workers’ compensation hearing, Bell worked primarily on two biopesticide projects, Laginex and Serenade.
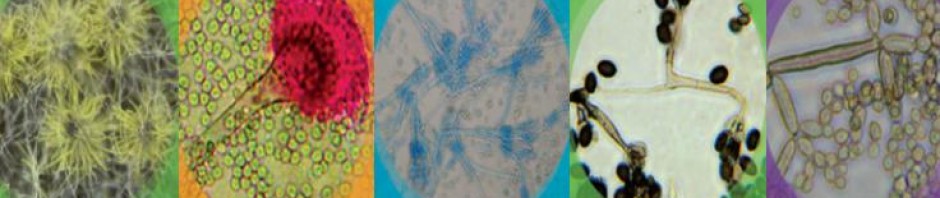
Laginex is the brand name of Lagenidium giganteum, a water mold (fungi), which infects and kills mosquitoes. In a series of experiments, Bell documented what happened in water with mosquito larvae and Laginex and how to lengthen the biopesticide’s shelf life.
Serenade is a biopesticide used to control insects on crops. Its active ingredients are the Bacillus subtilis bacteria, which AgraQuest first found in a Fresno peach orchard. Bell tested soil samples taken from locations worldwide, using a fermentation process to extract the bacteria. He and a co-worker filled 10-kilo bags of Serenade from a larger drum. Bell did not wear a respirator while loading the Serenade.”
At the March 18, 2008 Davis City Council meeting, the Davis City Council presented Pam Marrone with the 2007 Business and Economic Development award. According to the News and Review, “Marrone left AgraQuest in March 2006 to found Marrone Organic Innovations in Davis.”
Marrone declined to comment for the News and Review Story; however, in October 2002, they write:
“As recently as October 2002, Marronewrote that Serenade is “safe to workers and ground water,” in the industry journal Pesticide Outlook. At the workers’ compensation hearing, Denise Manker, AgraQuest’s vice president of global product development, testified that the company and its employees followed proper safety procedures and had tested its strain of Bacillus subtilis to ensure it did not contain a substance that causes allergic reactions. While noting that soil samples in the laboratory can be hazardous if handled incorrectly, she said it was highly unlikely that Bell had become infected by the Bacillus subtilis, since it’s not known to be harmful to humans.”
Doug Haney is an advocate for human and patient rights who specializes in mold and microbe exposure. He wrote a book entitled “Toxic Mold! Toxic Enemy!” In it, he argues that over the years many researchers and doctors have been skeptical about the possibility of micro fungi infection, however in recent years there is increasing evidence of the danger of such organisms.
David Bell visited the Mayo Clinic in Arizona and they discovered a whole range of possible infectious agents. Sandi Trend, Bell’s mother, was able to link many of the agents in the patents that AgraQuest was using to agents found in David Bell’s body over the course of the last decade.
“According to peer-reviewed articles in British medical journal The Lancet, and other sources, serious questions have been raised about the safety of Bacillus subtilis for humans and animals.
Tests conducted at the clinic determined Bell had histo yeast, a mold found in soil, in his blood serum. He had developed histoplasmosis, which according to the federal Centers for Disease Control and Prevention affects the lungs and other organs and can be fatal if not treated.”
Unfortunately, it does not appear that OSHA, the Occupational Safety and Health Administration is equipped to handle this sort of problem.
CAL-OSHA investigated AgraQuest and found three of its ventilator hoods did not meet state standards. However, this was unrelated to the problems that David Bell is suffering from.
One of the big problems was pointed out by esteemed Dr. Larry Rose, who was the last doctor that worked for CAL-OSHA. OSHA has increasingly relied upon industry doctors and more often they have simply looked at smaller technical problems. They simply do not have the expertise to examine and diagnose this sort of problem.
As Larry Rose pointed out during a video interview which also featured local Davis activists and author of “Death on the Job” Dan Berman:
“When you’re called in and a worker has possibly picked up a very serious infectious disease from the work process, you don’t just go in and measure a face velocity and give a tag. You’ve gotta do some… you know real investigation. Go over all the medical records and you’ve got to get the organism and submit it to the proper lab to determine it’s patogenicity. In other words, there’s a series of steps you would take because you’re not only trying to protect all the workers there now and future workers, but you also have to protect the community when you’re talking about an infectious disease, this is a serious public health matter. So looking at what OSHA did [and] I’m just astounded that they had that kind of very weak response, inappropriate response according to the law.”
THE THREAT TO DAVIS–BIOTECH LAB IN A RESIDENTIAL NEIGHBORHOOD
As Doug Haney pointed out to me early on in my examination of this potential problem, he would be much less concerned about the possible health implications for the surrounding community of Davis if he believed that the lab was properly contained from the outside environment. Instead both photographic evidence and testimony from David Bell lead us to the opposite conclusion.
“The 20,000 microbes that they boast had been discovered throughout the world… were not fully contained in a way that specialized laboratories would require. That means they were in drawers, that they were open at some point, and exposed employees to whatever they were, they were unanalyzed, they were not determined at any point as to whether they were dangerous or not dangerous. That type of thing tells me that the laboratory was not a well-kept laboratory. The other part of it is that the building was in a residential area rather than a specific area for laboratories over in the Davis area.”
The problem as Mr. Haney pointed out:
“[AgraQuest was] very soft in their application of training, in fact there was little or none that I know of that David [Bell] indicated. There were open suitcases of dirt or soil that had been brought in from foreign countries that were exposed in the laboratory. OSHA and other standards for laboratories indicate that you should not have any kind of drinks or foods associated in the actual work areas of laboratories, they have to be set aside, that wasn’t the case at AgraQuest.”


One of the biggest points of concern are photographs that show considerable corrosion on the outtake pipes several years after the lab moved from Kennedy Place to Drew Avenue. Is this residual pollution from the AgraQuest lab? Doug Haney believes so. As alarming was the fact that the dead crow in the picture above lay just beneath the pipe–undecomposed for two weeks between the time that the picture was taken and when Mr. Haney inspected the location.
“Ms. Trend had gone to that location about two weeks before I had a chance to view and told me about the fact there was this bird out there that was under this water outlet that showed a lot of corrosion, a lot of chemical build up. One thing about microbes, especially microfungi, is that they are the first to decompose in the external elements outside. This bird was not decomposed which told me that the company that produced the chemicals, Agraquest, were to destroy microfungi. And in this case, it kind of gave me the conclusion that those chemicals even six years after they had moved from the building were still strong enough and in the soil enough to eliminate rapid decomposure that rapidly takes place after an animal or person or a live species dies.”
It would be a fairly easy task to have an agency or the health department take soil samples from around this building and determine if this actually represents a threat to the health of Davis and whether or not AgraQuest was responsible for this contamination of the environment.
Another concern is accounts by David Bell that indicate the use of a type of drain as a place to dump chemical and possibly biological residues.

David Bell told the Vanguard by phone from his current residence in Texas:
“It was more like a concrete culvert that enters onto a lawn, I don’t think it actually goes into a sewer system. They chiseled out most of it already. It would kind of be like a big water runoff area, it was concrete and kind of sloped to the center, and that’s where the cleaning of everything took place.”
In the video that featured Dan Berman and Dr. Larry Rose, Sandi Trend, the mother of David Bell gave a full description of what occurred:
“David was instructed…. He was told to pick up this “drum” that was on an offsite farm because they wanted to use this drum for other broth, fermentation broth. So what he did is he went over to this farm and he brought it back and there was still liquid in it. So he didn’t really know what he was suppose to do so he was told to clean it out and dump it down the drain. What drain? Well outside the lab….. and I went up there after this because I was trying to visualize in my mind, he’s telling me that they mixed up powder in the bathroom and that the only ventilation was the bathroom fan, which is a normal household fan – ok. So I’m trying to visualize this and when I get there I’m going, “What drain”? And I wasn’t the only one that was there so there was somebody with me. It’s like “what drain” and “I don’t see a drain” and it’s like “Well I wonder if that’s what David’s talking about “? And what it was was it was like a storm drain, right outside the lab door that had just been hollowed out into the concrete and it led right into the dirt. So, when I called up David I go, “Is this the drain you’re talking about”? He says “yeah”. And excuse the expression… ok? I go “you dumped it out there”?! And he said, “that’s where we dumped everything”. I said, “what the hell did you do that for”? “That’s were we dumped everything Mom, that’s where I was told to dump everything”. So, right into the dirt.”
The Vanguard asked David Bell whether there were pathogens in the drums:
“There should have been by that point [live pathogens in the drum]. Everyone was arguing whether bacillus subtilus was pathogenic, however the fermentation process would get contaminated. If it sat that long there definitely could have been anything sitting in there. The fermentation process was still relatively rich in nutrients. So once it’s opened up to the air for the very first time things start in at that point.”
In addition to dumping drums in the ground, there was also loss of some of the specimens from the lab.
“We were losing mosquitos all the time until I came up with a system to hold them in a mason jar with a screen on it. We were actually losing mosquitoes that weren’t even endemic to our area in our area.”
What kind of mosquitoes I asked David Bell:
“In particular what we were releasing were the malaria mosquitoes. There was no way to keep them contained when I showed up there.”
He said he believed the number that were released was probably too small to allow them to reproduce, but nevertheless this is another example of the lax control standards at the original.
AgraQuest’s new location on Drew Street may in fact be much more secure and up to date in their practices. It is important to note that the OSHA violations occurred at the new Drew Street location rather than the original location on Kennedy Place. As far as anyone knows, OSHA never inspected the original lab on Kennedy Place.
Where does this leave Davis at this point? It is difficult to say. Someone needs to thoroughly examine the soil around Kennedy Place to determine whether or not the agents in the soil represent a health threat to the Davis community.
I asked Doug Haney how big a concern this was. He pointed out that scientists estimate there are roughly 1.5 million microfungi and other species that have not been discovered and we only know about perhaps 400,000 species. That means you have an area from a foreign country that has ben excavated, you have a lot of unknown factors here.
“When you excavate an area that has never been excavated before into a foreign country, you are bringing those microbes in a new area and what happens with microbes in order to survive, they either fight off or ward off other species, or they integrate with other species and hybrid the species which makes them far more dangerous. “
Moreover, these species can survive for long periods of time as spores or in dormant stages. The health implications are unknown but potentially very serious.
“You could possibly rise in say neurological diseases, a rise in lower birth rate, a rise in cancer, a rise in leukemia, a rise in serious diseases.”
These could show up almost immediately in some cases such as David Bell or they could could impact the population down the line. It could be 10 to 20 years before some of the implications of this are fully known.
Again, much of this is simply unknown because no responsible agency or regulatory agency has really investigated the matter. That is perhaps the most alarming aspect of all of this.
On October 1, 2007, Sandi Trend and Doug Haney met with District Attorney’s Office Investigator Dan Stroski. Mr. Stroski was immediately interested and alarmed, however, he informed them some time later that the Yolo County District Attorney’s office did not have the resources to do such an investigation.
The Vanguard will have a follow up article on this next Monday where we will examine the implications for how AgraQuest got these soil samples into the country and the potential threat that that represents.
—Doug Paul Davis reporting
Story – davisvanguard.blogspot.com
Note – This is the “undecomposed” bird I found in the fireplace of the mold infested apartment (Jefferson Lakes) leased to us by Riverstone Residential (mold they have been hiding for years and continue to do now). I can’t help but think of it as the “canary” that died from the toxins produced by such large amounts of mold. Maybe mold toxins also act as a preservative after death. katy

